- When can you use My Health Record?
- Do you need patient consent?
- What documents can you create and upload?
- What types of information can be viewed?
- How do you view documents from other providers?
- How do you view Medicare documents?
- How do you explain My Health Record to patients?
- How do you stop information being uploaded?
- Addressing GPs' concerns
- Penalties for misuse
- Training
- More information
When can you use My Health Record?
The My Health Record can only be used for the purpose of providing healthcare to a registered healthcare recipient (e.g. the patient or client). The patient need not be present when you access their record, as long as the access meets this condition.
Do you need patient consent?
No. Any person involved in a patient’s healthcare who is authorised by the My Health Record registered healthcare organisation, can use information from and upload to a patient’s record as permitted by the My Health Records Act 2012.
This can occur during a consultation, or outside the consultation without the patient being present, provided it is for the purpose of provision of healthcare.
The Australian Medical Association states that it is good medical practice to advise a patient that you will be uploading information, particularly if it might contain information that a patient may regard as sensitive.
See also the section on consent in the Shared Health Summary article.
What documents can you create and upload?
Depending on the capabilities of their clinical software, participating general practices can upload two key documents to the My Health Record:
- Shared Health Summaries - see the Shared Health Summary article.
- Event Summaries - see the Event Summary article.
General practices can also upload scripts if they are using an electronic transfer of prescriptions (eTP) product.
What types of information can be viewed?
Any information uploaded to the My Health Record can be accessed by healthcare providers in the provision of healthcare. The exception is a patient’s Personal Health Notes, which is purely for a patient’s own use and can only be viewed by them.
Information that is most commonly available in My Health Record include:
- Shared Health Summaries
- Event Summaries
- Medicines:
- Discharge summaries
- Pathology and diagnostic imaging reports.
- This is the current list of who is uploading pathology and diagnostic imaging in each State and Territory.
- Medicare overview
- Australian Immunisation Register (AIR) records
The following may also be available, though at this stage they are less common. They are expected to be more common as usage of My Health Record increases.
- Specialist letters
- Referrals
- Advanced Care Planning information
- Information about a patient’s past health events
- Child development information
- Consumer-entered information
- Pharmacist Shared Medicines List
How do you view documents from other providers?
There are summary sheets for a range of clinical software products with step-by-step instructions and screenshots for viewing a My Health Record:
The Australian Digital Health Agency has more information on how to view information in My Health Record.
How do you view Medicare documents?
My Health Records may contain up to 2 years of past Medicare data, such as:
- MBS items
- PBS items
- organ donor information
- immunisations included in the Australian Immunisation Register
Unfortunately, the filter settings in most clinical software don’t include Medicare data by default. You first need to change the filter to include Medicare Records. Here's how to see the Medicare section:
Medical Director

Best Practice
- Untick Exclude Medicare documents
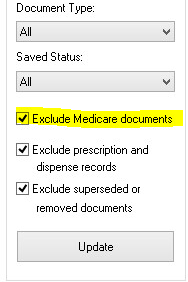
- An additional two Medicare reports will appear:
- Medicare overview – past 12 months
- Medicare overview – all
- Choose the relevant report and double-click to view
- This will display a report with PBS & RPBS items, AIR data, Organ Donor information & MBS & DVA items for the duration selected. Note: you might need to scroll to the end of the document to find the MBS items.
Pharmacy dispensing software
- Within the patient's My Health Record, go to the Clinical Documents section
- Click on the Medicare Overview (all records) document
- Scroll down to find the Australian Immunisation Register – AIR
How do you explain My Health Record to patients?
For patient resources see the article on promoting My Health Record to patients.
How do you stop information being uploaded?
If a patient has a My Health Record, pathology reports, diagnostic imaging reports and prescription records may be uploaded to that record. This will occur automatically, and it is not necessary for you to seek consent from your patients.
Pathology and Diagnostic Imaging
If you, or your patient in consultation with you, do not want a pathology/diagnostic imaging report uploaded, withdrawal of consent should be communicated using your clinical software or with a handwritten note on the request. Your patient can also communicate this verbally when presenting at the pathology or imaging laboratory.
The links below are to information for how to change the consent status for the upload of pathology or diagnostic imaging results
-
- Genie
-
- Zedmed
Prescription Records
Preventing a prescription from being uploaded must be done before the prescription is printed, as by that point it is automatically uploaded.
The links below are to information for how to change the consent status for the upload of prescription records:
Note: If the prescription has already been printed, then the consent status cannot be changed retrospectively. It will need to be deleted and re-prescribed with the consent status changed as required.
Confidential Items in Shared Health Summaries
Some of the clinical software products permit medical History items to be flagged as Confidential. This can be used to omit these items from a Shared Health Summary.
- BP Premier
- If a Medical History item is flagged as Confidential = Yes, then the column headed My Health Record changes to = No.
The item is NOT included in the Shared Health Summary. The confidential status will need to be changed for it to appear on the Shared Health Summary.
- If a Medical History item is flagged as Confidential = Yes, then the column headed My Health Record changes to = No.
- Medical Director
- If a Medical History item is flagged as Confidential = Yes, then item will appear in the Shared Health Summary with an “unticked” checkbox to avoid accidental uploading. You can still choose to tick the item if you desire to include it in the Shared Health Summary.
- Other clinical software: refer to your software user guide or contact your software vendor for support.
Addressing GPs' concerns
- Katrina Otto's Top 30 questions doctors ask about My Health Record.
- While it was originally called the Personally Controlled Electronic Health Record, “personally controlled” does not mean that patients can change data. They do have the ability to remove or hide a document, but they cannot change anything within that document.
Medico-legal questions
- View the RACGP webinar Medico-legal concerns and My Health Record.
- Read the questions and answers from a presentation for GPs on the topic held in November and December 2018.
Penalties for misuse
There are penalties for The Australian Digital Health Agency describes in detail the penalties for the misuse of health information.
The My Health Records Act includes the obligation to notify of an eligible data breach.
Training
The Australian Digital Health Agency has an eLearning portal for My Health Record and a training environment, which includes On Demand Training where clinicians can practice using a demo version of the same clinical software they use for work. Call your local PHN for advice on training.
Tips for On Demand Training:
- From the Online Training page, scroll down to the section headed “Get Started with On Demand Training”.
- Once you’re in the virtual computer, you will sign on to the software as normal. The password is: P@ssw0rd (that’s a zero, not an O!)
- If you have trouble connecting:
- Use a different browser (e.g. if you're using Chrome, switch to Firefox).
- Use another computer.
- Wait a couple of hours and then retry.
The On Demand Training resource also has a demo version of the patient’s view (which is called the Consumer Portal). Seeing what patients see may help doctors and nurses to talk to patients about it. Look for the section headed “Get Started with On Demand Training”.
More information
- The RACGP has useful resources about My Health Record.
- The Australian Digital Health Agency has information to help you learn about using My Health Record.
- Find out how to set up your access to the My Health Record system at the Getting started with digital health article.